
The Fleming Method for Tissue and Vascular Differentiation and Metabolism (FMTVDM) using same state single or sequential quantification comparisons.
As previously discussed, nuclear imaging began with Blumgart as he attempted to quantify the strength of the heart using circulation time using a Geiger counter.
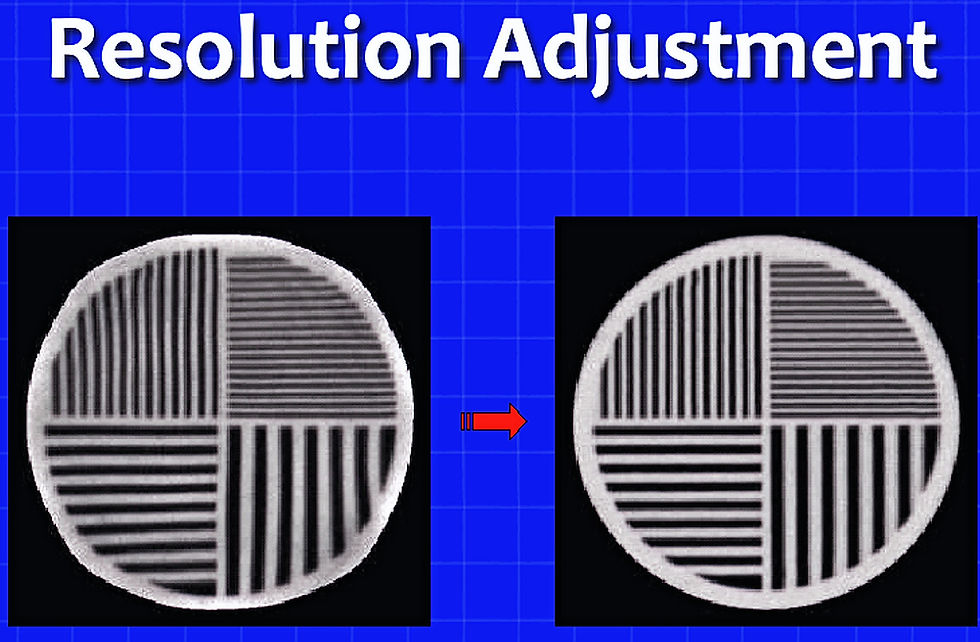
When nuclear imaging switched from the Geiger counter (a quantitative measuring tool) to modern nuclear cameras, the emphasis was placed on improving the appearance of what was seen with accuracy assumed.
The following image shows the progression of Nuclear Cardiology from Blumgart to FMTVDM.

By 2011, more than 10 million heart studies (myocardial perfusion imaging; MPI) were being done in the U.S.A. alone.
The errors present in these studies - shown in the following graphic - resulting from protocols with incorrect timing, excessive radiation exposure of patients, misinterpretation of images by physicians and allied health care providers, as well as errors in data collection by qualitative imaging, results in roughly 1/4 of the people being misdiagnosed.
The errors include missing critical heart disease while telling other people they need treatment, when in fact they don't.
The need to improve patient care by quantifying with FMTVDM - not to mention the need to simply improve the science of medicine - cannot be over emphasized.

To correctly carry out FMTVDM quantification of regional blood flow and metabolism involves a series of steps.
Before the person arrives for their FMTVDM study.
First, qualitative (quality) control (QC) of the nuclear camera using the steps we have always employed to assure visual uniformity and while this will assure visually appealing images, it does NOT guarantee that the images acquired are the result of accurate measurement of the isotope energy being disseminated from the patient to the nuclear camera.
There are different QC steps depending upon the type of nuclear camera you are using. E.g. planar, SPECT, PET, et cetera.


This ability to measure is critical when two images are being compared. For example, if you are comparing two sets of heart images to look for Coronary Artery Disease, or if you are comparing the results of any test from one laboratory to any other laboratory (hospital, doctor's office, city, country, et cetera), or if you are trying to determine if your treatment is working (before and after treatment results).
Second, quantitative calibration to assure the nuclear camera is actually measuring what is happening inside the person (or animal) being studied. This was discussed in the last tabbed page and is unique to FMTVDM (i.e. TFM component.)
After the person arrives for their FMTVDM study.
Third, the sequence of steps (order) must be carried out depending upon the type of FMTVDM study you are doing. One of the critical steps is the use of stressors - either physical or pharmacologic (chemical) - to produce enhancement of regional blood flow. This will occur throughout the body, including the area of interest (heart, breast, cancer, infection, et cetera). This also means that full body imaging cameras will allow complete body imaging with measurement of the person's state of health or problems, in roughly the same amount of time that would be required to merely look at one part of the body.
Fourth, the imaging must be performed at the right time, in the correct way, to find the problem you are looking for. If you look too early or too late, or in the wrong place, you will not find what you are looking for.
For my students I equate this to taking a picture of the Grand Canyon mid-day to capture sunrise, or having a lens cap on the camera when taking a photograph of your friends, or ... I think you get the picture! Which is after all the point - getting the picture, a useful picture that is meaningful. It will not impress your friends to take a picture of the Pacific Ocean and tell them it's a picture of the Serengeti. One has lots of water, the other none - they will not be fooled. It also will not impress the person undergoing diagnostic and treatment (theranostics) imaging if you don't follow the correct imaging protocol.
--------------------------
It is only when FMTVDM was used to find and measure the extent and severity of coronary artery disease - along with other health problems - that it became painfully apparent that these iatrogenic errors plagued nuclear imaging.
Each year approximately 225,000 deaths occur in the United States due to iatrogenic errors; now the 3rd leading cause of death behind heart disease and cancer - two of the critical InflammoThrombotic Immunologic Response Diseases we have been talking about.
The use of FMTVDM will therefore reduce the #1, #2 and #3 cause of death in the USA and around the world.
This use of FMTVDM to find and measure CAD is dependent upon FMTVDMs ability to measure changes in regional blood flow that occur between the Enhanced (Maximal) and Baseline (resting) states of blood flow.
These differences in flow reserve (CFR, SFR, FFR) can be measured/quantified by FMTVDM and are simply the
maximum flow (Q)
baseline flow (Q)

These changes in flow can be compared not only between the different coronary arteries; but, also between the outside (epicardium) wall of the heart where blood flow will be impaired last AND the inside (endocardium) wall of the heart where the smallest blood vessels occur.
These endocardial blood vessels are both furthest from the main (epicardial) coronary arteries and under the greatest pressure from both the squeezing action of the heart (cardiac) muscle and the blood inside the left ventricle being compressed by the heart just before being ejected into the aorta to go to the body.
As a result, the endocardium will, in most instances, be the first area of the heart to be compromised and be damaged (infarcted) should blood flow through a coronary artery be impaired.
The ability to measure (quantify with FMTVDM) instead of visually guessing (qualitative) is critical.

It should go without saying, but I will say it here anyway, every and I mean every person who undergoes FMTVDM, should understand the risks and benefits of doing so.
The primary risks are no different from any other nuclear imaging test. The difference is the intelligence applied to the imaging on the part of the people doing the FMTVDM.
Nuclear cameras have to be calibrated both for pretty pictures (qualitative) and for accurate (quantitative) results. These quantitative results are then analyzed and interpreted based upon actual data, not what someone thinks they see.
People can have problems from bleeding (you are sticking something through their skin into a vein), infection (you are sticking something through their skin into a vein), allergic reaction to the isotope and pharmacologic enhancing (not actually stressing the body but the terms die hard) agent being given, or the effect of the pharmacologic enhancing agent (increased blood flow everywhere in the body will be interpreted by people differently but it will wear off during the study or it can be reversed if needed; or the antidote is usually a cup of coffee, tea or caffeinated soft drink).
The nuclear camera could fall on you - don't laugh, it's happened. Again, not FMTVDM's fault but then it wasn't during an FMTVDM study. It was one of those qualitative pretty picture studies.
BENEFITS: Figuring out what is happening inside your body and deciding what to do about it and as we have seen, finally knowing if what you are doing is actually working!
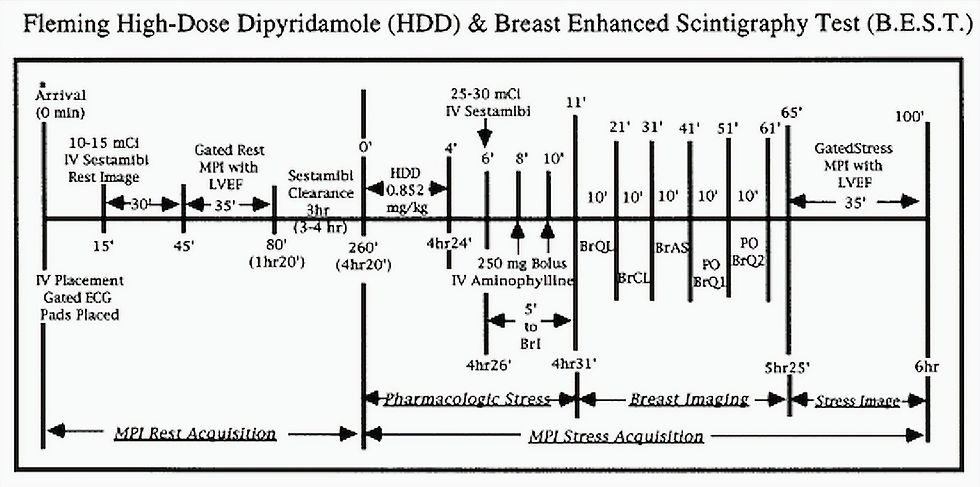
While the exact protocol (sequence of events needed to be carried out) for any given FMTVDM study will vary depending upon the nuclear camera being used, the nuclear isotope being used and what you are looking for; the following example is one of the protocols laid out to look for
Heart Disease,
Breast Cancer,
Lung Cancer,
Thyroid Cancer,
Parathyroid Cancer, and
Thymus Gland Activation - e.g. BAA
[Bacterially Aggravated Atherosclerosis]
after the person is given a lovely gown and asked to lay down on the padded imaging table.

Enhancement versus Stress
The term stress (test), started to be used when Dr. Bruce developed the treadmill exercise test to produce angina and electrocardiographic changes in people with CAD. He and others since have called this stressing the patient.
Unlike pharmacologic enhancing agents which relax the coronary (and all) arteries, allowing them to dilate and increase (flow reserve) the amount of blood flowing through them, treadmill stressing (old terms die hard) actually increases the blood pressure and narrows the coronary arteries. It does; however, actually stress the patient and as a result, some people will either have a heart attack or stroke during or following their treadmill test.
As the Harvard Medical School pointed out on its website, treadmill tests tend to be abnormal when there is a 70% narrowing of the coronary artery and usually require additional testing for confirmation.
As discussed previously, 80-85% of all heart attacks occur in people who have InflammoThrombotic Immunologic material built up in the walls of their coronary arteries, with little or no narrowing of the coronary artery lumen, where the blood is flowing through the artery.

For people allergic to the pharmacologic enhancing agents, or who just want to see what they can do on a treadmill, there is always that option.

Determining Baseline or Rest
The term rest became popular when BigPharma convinced physicians, and the world, that their isotopes were essentially static. That once these imaging isotopes are injected into us, they are taken up by the cells of the body and do not move around; in other words they do NOT redistribute. Isotopes that do move around are said to redistribute.
However, if you are looking at a visual (qualitative) image and looking for differences, you wouldn't notice any change if the blood flow and cells were working normally because the isotopes would be taken up and released and taken up and released; over and over again.
The claim made by BigPharma, that some of their isotopes - particularly the technetium-99m (Tc-99m) isotopes that generate massive amounts of money for Big Pharma - do not move around (redistribute), means you have to buy and give the patient more than one dose of radioactive isotope.
As FMTVDM was being developed, and isotope movement (redistribution) was being measured following the 5-minute image simultaneously obtained with the breast cancer (BEST) imaging, and then compared with the 60-minute heart image, it was discovered that the Tc-99m isotopes do in fact redistribute. This is only seen if there is heart disease.
When the heart disease is critical - severely reduced blood flow and potentially impaired heart cell metabolism - there is a delay in the uptake and release of the isotope. FMTVDM was able to measure this effect and I called this "washin" as it takes time to "wash in" to the area. Unfortunately, as I have presented at medical conferences; later joined by others including the South Korean research confirming this, this means that waiting for BigPharma's recommended 1-hour to image the patient, means we miss critical heart disease. One more iatrogenic error added to the list and in too many instances one more dead patient.
If there is no heart disease, the isotopes are taken up and released, taken up and released, over and over again. To detect the subtle difference that occurs as the isotopes decay (lose their radioactivity) requires quantification, which FMTVDM provides.
Finally, if there is CAD, but it is not critical, there will be uptake of the isotope from the blood into the cells of the heart. However, these cells will not function as well as they should because of their impaired blood flow. As a result, they will begin to take up the isotopes, only to lose it more rapidly than health heart cells. This greater than expected loss is called "washout" as the isotope washes out of the cells more rapidly than expected.
The following graphic shows early results measuring and exposing this lie by BigPharma. As you will see under the "Overview Videos" - "Big Pharma Lies" this was not the first time BigPharma lied about the redistribution properties of isotopes.

While this denial of Tc-99m isotope redistribution by BigPharma, resulted in physicians and hospitals around the world following the recommended delay in imaging after injecting these isotopes, allowing time for the isotopes to be taken up by the heart; this redistribution denial and required delay in Sestamibi uptake was used by BigPharma as a marketing tool, encouraging Physicians and nuclear technologists to wait - freeing up time and resources in nuclear laboratories.
This became a major marketing tool for Sestamibi over Teboroxime, resulting in the almost exclusive use of Sestamibi alone.
Following a failure by the federal government to intervene - perhaps because of the relationship between the FDA and BigPharma - I submitted my concerns to the attorney general for the state where Sestamibi's BigPharma Company was headquartered - New York.
The attorney general for New York, Latitia James, refused to investigate further after she received the following respone from the FDA and the Center for Drug Evaluation and Research (CDER).
This response should have initiated an investigation and prosecution by Ms. James, as it confirms what I said.
1) Sestamibi redistributes, and
2) Based upon information provided to physicians, imaging was delayed past the time when critical heart disease woudl be found.

Helvetica Light is an easy-to-read font, with tall and narrow letters, that works well on almost every site.
Perhaps more important than the misrepresentation about the isotopes redistribution characteristics - although it's hard to downplay the significance of the additional sales of tens of billions of dollars in isotope, 3-million extra curies of radiation given to patients along with additional radiation exposure to those involved in the nuclear imaging studies, and the countless numbers of errors made in misdiagnosing patients through the incorrect timing of imaging - is the actual issue of the timing sequence BigPharma reported to the FDA.
As the above communication clearly shows, BigPharma specifically stated that the standard of care is to begin imaging the heart 15 to 60-minutes after the isotope is given. An imaging standard of care promulgated by BigPharma that perpetuates the lack of redistribution fallacy continuing to plague the qualitative imaging approaches.
In fact, it would plague FMTVDM, if you waited too long to see the problem - and 15-minutes is too long to see critical heart disease.
Which injected dose of the isotope are you seeing?
The final consideration in this stress-rest two injected doses of isotope approach is the term rest and the inability to differentiate which dose of injected isotope you are seeing. Are you seeing the first dose injected following stress or the second dose at rest or some combination of the two. It is impossible to distinguish what you are looking at when you give to injections of the same isotope. The introduction of more iatrogenic error.
All of this speaks to the importance of knowing what the isotope you are using actually does. What determines the uptake, release and subsequent measurement of the isotope?
Errors introduce flaws, flaws introduce mistakes, mistakes lead to misdiagnosis, injury and potentially death.
Tonight, when you go to sleep, you are truly experiencing resting blood flow to the heart. However, we don't do imaging studies on sleeping patients and once you wake up - even if you are just laying in bed - your metabolism and thus the regional blood flow to areas of your heart has changed. It is no longer at rest, it has increased.
Therefore to use the term rest is a misnomer. You are for all intensive purposes, once awake, at baseline - not rest - and it is this baseline regional coronary blood flow that we want to quantitatively compare, with your enhanced regional blood flow.
To do this accurately requires that we be able to quantify the amount of isotope delivered through the coronary arteries to the heart muscle, both at enhanced and baseline conditions.
This cannot be done accurately if part of the isotope from one part of the study is still present and being measured during another part of the study when you have given more isotope.
Hence, The Fleming Method for Tissue and Vascular Differentiation and Metabolism (FMTVDM) using same state single or sequential quantification comparisons.
Routinely people given the same isotope twice, justify their ability to distinguish between the two doses by saying sufficient time has passed between the stress and rest studies.
However, since the isotope redistributes - and even if you somehow still bought the argument that the isotopes don't redistribute and remain in place - residual isotope from the first injected dose will be present in the heart. This means, when you give the same isotope a second time, you cannot distinguish between the first and second injected dose. The result, of what you think you see on the second study, is contaminated by the first injected dose.
If this is confusing, let me use the following example. If I let 30-llamas run (stress) into a field and begin eating, and 10 of them wonder off there will still be 20-llamas left in the field. If I then let 10-more llamas causally walk (rest) into the field and after a while 5-llamas wonder off there will still be 25 llamas in the field. How many of those llamas are from the first group and how many are from the second group?
Accepting any error when someone's life is on the line is unacceptable. Accepting the errors of not quantitatively calibrating the nuclear imaging cameras, of sacrificing information for visual appearance (pretty pictures), of contaminating one image result with the left over isotope from another imaging effort, of incorrectly defining what we are actually looking at (stress versus enhancement; rest versus baseline), and of not actually measuring the results of the imaging studies, are all examples of a seriously flawed system promoting BigPharma over patient care.
FMTVDM Quantitative Imaging
As shown in the example protocol above, once the patient has been prepared for FMTVDM imaging (informed consent, fasting, lovely gown, IV in place, et cetera) the study is ready to begin.
Prior to this, decisions - as I have mentioned - to be made. What are we looking for? What type of nuclear imaging camera are we using? What enhancing agent or method are we going to use? What isotope are we going to use? What is the redistribution timing of that isotope? This redistribution is factored into the FMTVDM equations used to measure flow reserve and ultimately AI derived narrowing or absence of narrowing.
Based upon the answers to these questions, the nuclear imaging camera will have been quantitatively calibrated and prepared for the patient and their FMTVDM study.
The timing of the enhancing agent and introduction of the isotope into the vein of the patient is included with the FMTVDM license, to guarantee that the FMTVDM study done in Los Angeles will be done exactly the same way it is done in Toronto, Paris, Wuhan or Timbuktu.
Accurate, Consistent and Reproducible.
Once these preparations have been made, and the patient is ready, FMTVDM can begin. Monitoring of vital signs and use of an electrocardiogram to detect any potential changes suggestive of insufficient blood flow to the heart are continued throughout the study.
Based upon the selected imaging agent, camera and enhancing agent - the study will begin by giving the enhancing agent through the IV followed by the isotope.
Initial (enhanced) and final (baseline) imaging - and subsequent measurement of the isotope after the patient has left - is based upon the peak enhancing effect of the enhancing agent as well as the redistribution properties of the isotope.
A few examples of isotope redistribution and half-lifes are shown in the following table. These are ultimately used in the computation of expected changes in isotope, versus measured changes in isotope, from which flow reserve and other calculated measures are made.

Once the enhanced and baseline images have completed, the IV catheter is removed and you can surrender that lovely gown in exchange for your street clothes. Further processing of the results, including FMTVDM measurements are completed after the person has left the imaging site.